

Technology and medicine have been interlinked with each other for a long time; this integration of tech with medicine has proved to be phenomenal. However, this very integration has caused some grave issues and accidents, one of which is the case of the THERAC-25.
What was THERAC-25?
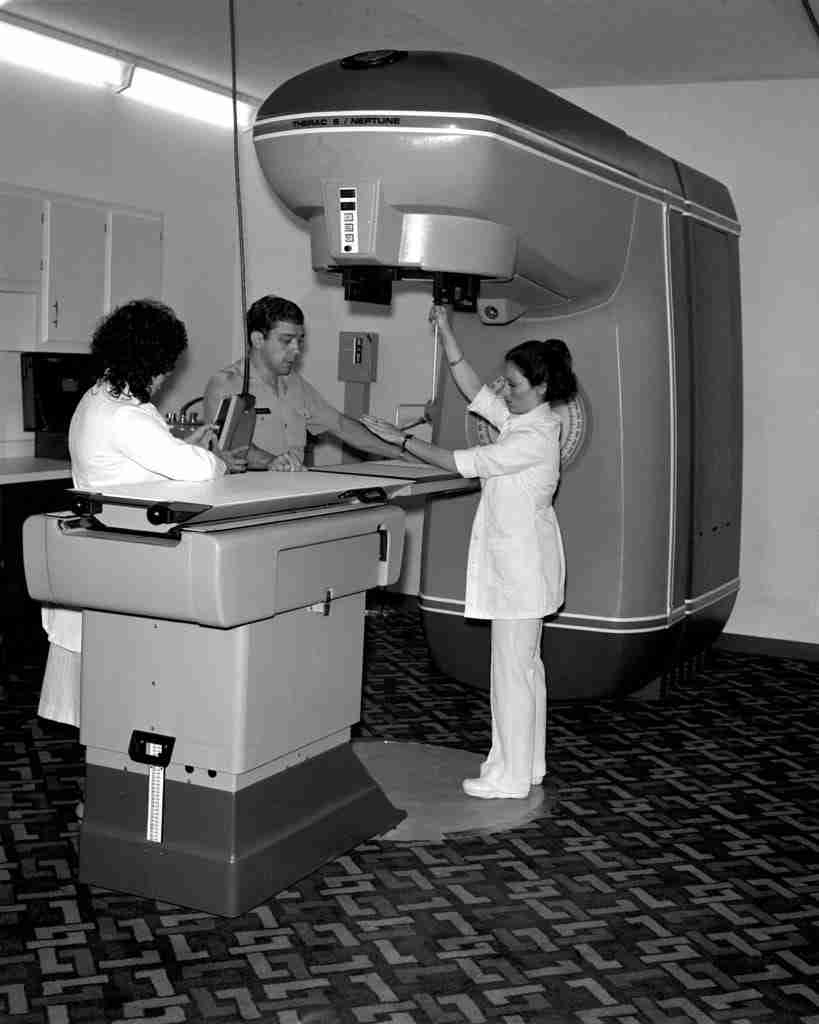
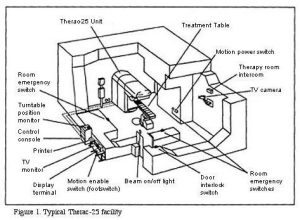
THERAC-25 is a computer-controlled machine created by Atomic Energy of Canada Limited (AECL) in 1982. This machine was used in cancer treatment by positioning linear beams of photons (X-rays) or electrons onto the affected cells. This machine was part of a series under the same name, with predecessors named THERAC-6 and THERAC-20, which were hardware-based linear accelerators, while THERAC-25 was software-controlled. Although it was equipped with supposed “safety mechanisms,” it led to many catastrophes.
Cases
In early June 1985, a woman named Katie Yarborough, who was undergoing cancer treatment at Kennestone Regional Oncology Center in Marietta, Georgia, went to get her usual radiation therapy. The state-of-the-art device, THERAC-25, was being used at the hospital. During the treatment, she felt a ripping-hot burning sensation that later turned into a disk-like shape on her back and left her right arm burnt. This was not possible, as the radiation levels were 200 rads. Upon complaint and later with the burn marks, it was brushed off. It was later discovered that Katie had received a dose of 15,000 to 20,000 rads.
The use of the machine remained constant, and another case surfaced where a 40-year-old woman receiving cervical cancer treatment was hit with 17,000 rads of beam on her left hip. She died of cervical cancer, but it was later revealed that her hip would’ve needed replacement if she had survived.
There are many cases; however, the worst of them is that of Ray Cox. He was a man undergoing treatment after the removal of a tumor from his back. As usual, he was sent into the room, laid down, and the technician began their work on the other side. Cox was hit with a flash of light; he began writhing in pain, but the intercom was broken that day. The technician learned about Cox’s condition when he banged on the door with his fists. Ray
Cox passed away after vomiting blood, experiencing spinal inflammation, and developing herpes simplex skin infections over the next five months. He was overdosed.
Malfunction 54
When the reports were made about the cases and the malfunctioning of the machine, AECL brushed it off by saying that it could not be a software or hardware failure, but rather an operational one. They kept brushing it off until the cases reached the FDA, where officials instructed the company to create a proper repair roadmap. AECL identified the issue with the turntable position, where the patient had to lie, and it was fixed. Many physicists insisted that the beams hitting the patients could not only be photons, as the machine was also capable of emitting electrons and X-rays, but they were faced with similar rejection by the company. As the fear wore off, THERAC was back in use. However, the cases were growing more gruesome, and since this machine was being used by hospitals all over the state, doctors and technicians began talking. One thing everyone found in common was a Malfunction message with a number from 1-64 in all the machines. One of them was Malfunction 54. Technicians became so desensitized to this message that instead of paying attention, they would press “P” or proceed to activate the machine. This later turned out to be a grave error.

Malfunction 54 & Hardware
THERAC-25 used a code that was adopted from THERAC-20; the problem was not this. The underlying cause was that THERAC-20 was coded by a man whose identity remains anonymous. He was an employee at the company and a hobbyist coder. The entire program was coded by him with minimal reviews. When it was discovered that the issues were with the software, testers found grave errors in the code, but the entire code of 100,000 lines was not reviewed, leaving flaws. In theory, THERAC-25’s mechanisms were perfect, but problems arose when the hardware interacted with it. The machine used two magnets to filter the beam, and it took 8 seconds to move the magnets. During those 8 seconds, if by mistake any changes were made on the screen controlling the machine, they were not detected. That happened with Cox; he was not hit by photons, but rather X-rays, as the technician accidentally typed “X” in the type bar.
THERAC was taken back, and the public was advised not to use it while it underwent safety measures, which later proved to be useless.
Another problem was that the code did not efficiently interact with the hardware, resulting in beams that were higher than intended while the screen showed the prescribed amount. The company fixed software errors while acting aloof toward Malfunction 54. Malfunction 54 was a software bug; it created a race condition that no one knew about except the company, who failed to educate people about it.

Ending of THERAC-25
THERAC-25 was proven to be flawed, and the company discontinued it. The same principle machines are still in use, but with better codes. THERAC-25 remains the worst software failure, causing 6 fatal accidents and leaving many people disabled. AECL refused to believe in Malfunction 54, deeming it impossible. The lawsuits were settled out of court, and that put THERAC-25 to permanent sleep.